
Copyright held by The John Cooke Fraud Report. Reprint rights are granted with attribution to The John Cooke Fraud Report with a link to this website.
Healthcare? Worker’s comp? Auto accidents? Slip and falls? Insurers survive and thrive because of their ability to sort the valid from the invalid, the real from the fabricated, the medical necessity from the medical build-ups. If you’re an adjuster, an SIU specialist, an attorney — any individual who relies on the ability to read medical reports with more than just a passing understanding of what you see — this new JCFR column is for you. Our author is an orthopedic surgeon who proudly “swings both ways.” He’s supported plaintiffs and he’s supported the defense. He has no connection or allegiance to either side. The body, he says, speaks for itself. The trick is in understanding the language it speaks.
And with that introduction, we are bringing you the second installment of the “Ask Doctor Bob” column.
—————————–
To all those who took the time to send questions, thank you. I’m sorting them into categories and will try my best to get to them all eventually. I’ve taken the liberty of combining some of your questions to allow this column to cover more territory. Keep them coming, please.
Q: When there is an attorney/clinic relationship and I get massive amounts of diagnostics, how do I determine what is appropriate and what might have been ordered strictly to build the medicals?
A. This was a repeated concern from readers. Most of you speak the language of claims handling; but I speak the language of medicine, so allow me to bolster your vocabulary with my own. Take a good look at the initial medical report, comparing the patient history and the doctor’s physical findings at that first encounter with the treatment plan. The time frame between the initial treatment provided and the ordering of any specialty tests is important. A sure red flag of an intended medical build-up is the early ordering of EMGs, CAT scans or MRIs for a patient with a soft tissue injury. Remember, if the injury is only to the soft tissue — strains or even sprains — it will present with minimal neurological symptoms; and it’s the presence of those neurological symptoms that supports the necessity for more extensive testing. A patient with no neurological symptoms does not need an immediate — and cost-building – – MRI. In my medical/legal experience, medical mills generally work under the assumption that nobody at the claim intake level knows what they are doing. The producers of these history/exam reports — often not the physician — do a miserable job with the initial report. Their intent is simply to bury the adjuster in a lot of hoo-hah: buzz words that look real but that actually relay little meaningful medical information.
When a mill relationship is inferred, it’s generally not only between the attorney and the physician or chiropractor. The relationship will usually extend to the treatment facilities as well with their large built-in profit margins. These details require early attention rather than the much later investigative attention when the file is 10 inches thick.
Claims intake processes that concentrate on only certain red flag indicators (while ignoring others) are easily defeated. The larger medical mill operations are continually revolving the names of their treating physicians or chiropractors by hiring new people who are transitioning from student status (where they have accrued huge student loan obligations and need money fast) to joining or establishing a real practice of their own. The mills use these people, their names, their pharmacy numbers, to circumvent insurers’ established systems. Personally, I avoided ever having to work in a medical mill. My first money-producing medical job was taking gonorrhea swabs for the County VD clinic.
Q: What influences a reasonable length of soft tissue injury recovery time and what are the variables?
A: The truth is that there really are no applicable standards; yet these non-existent “standards” are often used to establish how long it should take for a particular patient to heal. The literature says that a simple strain injury should heal in six to eight weeks; however, that same literature seldom addresses the fact that no two human beings are exactly alike. An active 20-year-old in good health, with no genetic aberrations, will experience a completely different healing time/process than a 65-year-old with a poor genetic background, diffuse arthritis, minimal activity, poor muscle structure and possible medically complicating conditions. There is no real standard.
This is where Med School 101 comes in. Let’s look at soft tissue injuries, beginning with three tissue types: muscles, tendons, and ligaments. Many other tissues may be involved in an injury; but to keep this simple, these are the main players in most soft tissue injuries. (No broken bones, etc.)
Muscle is a highly vascular tissue that heals quickly. Vascular means the tissue has excellent blood circulation, oxygen saturation and overall hydrating/healing ability. But all tissue changes with age, lifestyle, nutrition and dozens of other variables. What was the medical condition of the patient pre-incident? Are we talking about Bill, a 20-year-old with high elasticity, good muscle tone, good vascular supply and minimal previous injuries? If so, healing would reasonably be rapid. Or was it Walter, an 80-year-old with one foot in the grave and the other on a banana peel? In Walter’s case, healing might be more of a challenge. So age is a giant variable.
Let’s compare two 35-year-old males. Lou is a construction worker who continually challenges his muscles, creating micro tears through strenuous activity. These tears continually repair themselves with relatively inelastic tissue. Over time, micro tears cause more inelasticity, compromising the normal physiology and slowing the healing process. (To simplify, the muscle tissue becomes “tougher.” ) Lou also continues to work, so the healing process may be slowed by the ongoing day-to-day re-injury to the tissue. Lou’s expected healing time is longer than that of the healthy 20-year-old Bill and actually creates more complications in his clinical presentation.
Jack, our other 35-year-old, has a sedentary job; he sits all day at his computer, doesn’t participate in active sports after work, and has lost much of his normal initial tissue function due to inactivity. (As they say, “Use it or lose it!”) Muscle tone is lost; muscle strength is decreased; range of motion is more limited; blood supply is decreased. But, amazing as it may seem, Jack’s recovery time will be shorter that Lou’s.
Why is this? Primarily because of the involvement of tendons and ligaments in soft tissue injuries. Tendons connect muscles to bones. These avascular tissues have no blood supply and instead eat by a process called inbibation — similar to a sponge — squeeze in, squeeze out. Movement is mandatory for tendons to heal. Lou’s activity level will help the tendon structures heal. Jack’s tendon healing will be slower because he doesn’t maintain his normal activity.
Then we have the ligaments, which attach bone to bone. Their overall purpose in the human body is to restrict motion. Ligaments are also avascular tissue. They eat/stay healthy by that same process of imbibation. So although Lou is able to provide the necessary movement to help the ligament heal, at the same time, his lifestyle continually stresses the injured ligament. The ongoing — and more difficult — cellular process of healing may cause hypermobility. Because of his sedentary lifestyle, Jack (1) is less apt to encounter hypermobility as part of his healing process of the ligaments and (2) will heal slower — but more completely. Two people and three tissue types (muscles, tendons and ligaments) produce six different curves. Yes, it’s initially confusing, but when you grasp the concept, it becomes almost … predictable.
Now let’s look at the 65-year-old, Stan — after which I promise to quit confusing you with names. Stan’s muscle tissue has a 65-year tradition of being micro torn and replaced with inelastic tissue. It could be from work; or it could be from mowing the lawn, walking the dog or wrestling with the kids and then with the grandkids. It’s just from the cumulative process that we call life. When Stan has an accident, his muscle (because of cell age) has both decreased elasticity and decreased vascularity. Stan has also had 65 years to experience previous insults to his system — he may have restricted motion and response time. At the time of the actual injury, Stan is less able to respond at the same speed as 20-year-old Bill would respond — or as Lou or Jack would. Why? Because he has less elasticity. What’s changed is that the muscle tissue itself has changed in character. It’s more, for lack of a better word, “sluggish.”
has an accident, his muscle (because of cell age) has both decreased elasticity and decreased vascularity. Stan has also had 65 years to experience previous insults to his system — he may have restricted motion and response time. At the time of the actual injury, Stan is less able to respond at the same speed as 20-year-old Bill would respond — or as Lou or Jack would. Why? Because he has less elasticity. What’s changed is that the muscle tissue itself has changed in character. It’s more, for lack of a better word, “sluggish.”
Look at your own hand and pinch the skin. If you are 20, the pinched skin will snap back. If you are 40, it will snap back, but at a much slower pace. If you are 60, it stands up pinched on its own for a while and then eventually goes back down. If you’re 80 —- it will still be standing on it’s own tomorrow. Why? Because as we age, the cells are genetically programmed to age just like the entire body ages. In the hand example, it’s the influx of collagen into the skin that causes the slowness of the skin response.
Now apply this rather narrow hand example to an entire body structure. And then add the fact that over the time period from being 20-year old Bill to being 65-year old Stan, our joints deteriorate based on usage and trauma — and (although it’s a whole different subject for another column) all these pieces combine to show you that there is no “norm” between any two people. Our bodies are the sum of our experiences and insults and of our genetic makeup.
I’d like to insert something here because it’s important. We can throw out statements like “takes six to eight weeks to heal” from now until next Tuesday; but if/when a case goes to court and the defense IME doctor says the seemingly obvious, the claimant attorney will invariably make it very clear that there are no credible peer review studies to support a time definitive statement like “It should take six to eight weeks.” And he is correct in that statement. None DO exist because norms do not exist. Bodies are like fingerprints: the variables are endless. Age, occupation, lifestyle, (smoking?), habits (proper hydration, rest, nutrition, posturing, exercise, etc. ad nauseum) all play a significant part in repair.
Q: I understand that structure dictates function and function dictates structure. Then how do genetic changes in structure/function affect treatment, healing , duration and reestablishing normality as close to possible?
A: Read the next sentence three times if necessary — until you completely get it. Any genetic alteration of normal structure complicates healing from a traumatic event that affects the area of changed structure. The structural change, be it bony or muscular or vascular, is going to complicate the healing process. How about using something simple here, like arthritis? Cumulative arthritic changes are accelerated with altered structure.
To illustrate, let’s momentarily go completely away from bodies and tissues and instead let’s talk about a car. You have three tires that are fine and one tire that’s out of balance. You can still drive the car, you can still do everything you always did, but that unbalanced wheel in the front is stressing all the mechanical parts that deal with the suspension, increasing the wear rate, and shortening the life span of multiple components of the vehicle. So even though you can continue to drive, multiple systems are experiencing failure. Bearings are overloaded, tie rods are overloaded, shock absorber life span is severely diminished, tire tread is wearing off at a much faster rate … and all of that, in turn, affects the functioning of the whole car. Even though the start of it all, the one bad tire, is only a small part of a much larger machine. That car is your body.
When considering a traumatically induced injury, a structural genetic abnormality changes everything as it applies to “normal” healing processes. It changes the way muscles are designed around the area and how weightbearing structures are designed in that area, and it changes the stresses that you have on those areas.
processes. It changes the way muscles are designed around the area and how weightbearing structures are designed in that area, and it changes the stresses that you have on those areas.
Let’s consider the person who has scoliosis, a lateral deviation of the spine. “George” is in a car accident. (I lied about no more names to confuse you.) Whereas a “normal” person might not be affected in a particular low impact collision, George has an inherent weakness that makes him more susceptible to injury. Muscles, ligaments and tendons are changed in a scoliotic patient — the larger the degree of scoliosis, the weaker the spine because of all the changes that have taken place in the structure to compensate for the initial abnormality. George’s recovery would be expected to take longer and to be more involved — no matter his age. Again, no two people are identical, and genetic abnormalities are far more common than you might think.
Q: As a physician, what are your feelings about the concept of IMEs.
A: Danger, Will Robinson. Danger, danger, danger. I do, however, have a rather strong opinion which I will share — and the reason for that strong opinion will become clear very quickly.
My experience is that there are two types of IMEs. The first is a paper IME in which the patient is never seen, essentially a physical medical records review by an educated, credentialed, medical practitioner. It’s very difficult for the reviewing doctor to give a definitive opinion without physical interaction with the patient. Believe me, I know, because I’ve done many.
The questions that need to be answered are never in the records because it’s simply too laborious to document everything in the written records. The history of the incident, which is the most important part, which sets the framework for the remaining evaluation, is usually very limited in scope. If the injury was sustained in an automobile accident, the injured party’s exact posturing pre-accident can make a world of difference in what gets stretched, pulled, broken or worse.
My best example here is the biomechanical aspects of what is generally referred to as a Tbone. The forces on the body change radically depending on where in the side of the car the impact occurred and the directional vectors. If you are hit sideways, straight on, there is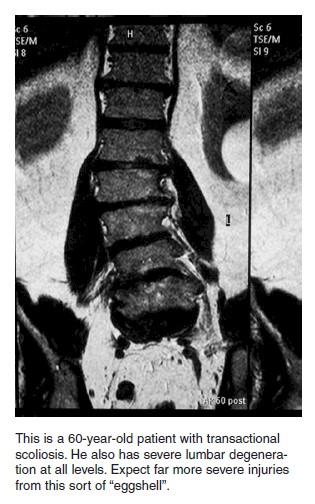 lateral flexion of the cervical spine. If you are hit at the front right axle, there is a total transfer of impact into the vehicle and rotation is added to the vectors of force. Three inches and 10 degrees can make all the difference in the world; yet that is never shown in the written records. So my answer on paper IMEs/reviews is that they are a good idea to get a general feeling of the patient’s response to treatment or if additional testing or alternative treatment is necessary. Period.
lateral flexion of the cervical spine. If you are hit at the front right axle, there is a total transfer of impact into the vehicle and rotation is added to the vectors of force. Three inches and 10 degrees can make all the difference in the world; yet that is never shown in the written records. So my answer on paper IMEs/reviews is that they are a good idea to get a general feeling of the patient’s response to treatment or if additional testing or alternative treatment is necessary. Period.
The second is the face-to-face IME: doctor/patient. The biggest problem here is that the IMEs generally take place at the end of treatment, not during the course of the treatment, and they are answering the questions, “Has the patient reached maximum medical improvement?” and “What are the residuals?”
A properly performed IME should combine a full review of all records prior to the visit; and it should involve at least an hour of face-to-face examination time. It will produce a detailed evaluation of the patient’s condition after a physical exam of the area of injury. A legitimately done IME correlates the history, physical findings, treatment regimen and residuals. It validates the entire process and is an excellent tool toward a fair result. The key word is this sentence is “legitimately.” The IME can also be a very powerful tool to identify those cases that contain elements of fraud.
Now comes the tricky part. I had the unique experience of being on the other side of the fence about 15 years ago; I underwent an IME in which I was put into an exam room, with a window, and then watched the doctor talk to an attractive prosthetic saleswoman, ignoring me completely, for 45 minutes of my booked hour. When he eventually entered the exam room, it was instantly apparent that he had no knowledge of anything beyond my chart name. He never physically touched me, and our face-to-face was no more than five minutes. A week later he submitted his “report.” He expounded on a lengthy physical exam and a full review of the records, and he opined that I had no residuals.
It irritated me sufficiently that for a period of time I went with my own patients to their IMEs. (It is permitted by my state law that patients have the right to have an observer in the room with them during their evaluation.) In every case I did this, despite the law very specifically allowing it, the IME physician refused to do the exam with a witness. Not some, not most, ALL.
Adjusters accept reports as if they are true; sometimes — make that most times — the fairness and medical inclusiveness of these reports is questionable. Personally speaking, I did hundreds of IMEs, spent a minimum of one hour face-to-face with each patient and never produced a fabricated report. Was I the exception or the norm? And was the physician who “examined” me for five minutes, without touching me once, the exception or the norm?
Dr. Bob is an Orthopedic M.D./Surgeon (retired) educated at ASU and USC.

