
Copyright held by The John Cooke Fraud Report. Reprint rights are granted with attribution to The John Cooke Fraud Report with a link to this website.
Healthcare? Worker’s comp? Auto accidents? Slip and falls? Insurers survive and thrive because of their ability to sort the valid from the invalid, the real from the fabricated, the medical necessity from the medical build-ups. If you’re an adjuster, an SIU specialist, an attorney — any individual who relies on the ability to read medical reports with more than just a passing understanding of what you see — this new JCFR column is for you. Our author is an orthopedic surgeon who proudly “swings both ways.” He’s supported plaintiffs and he’s supported the defense. He has no connection or allegiance to either side. The body, he says, speaks for itself. The trick is in understanding the language it speaks.
And with that introduction, we introduce the “Ask Doctor Bob” column. (And herewith confess that this month’s questions are plugs.)
Dear Dr. Bob;
Can you explain the difference between a bulging disc, a ruptured disc, and a herniated disc?
Andy Adjuster
Dear Andy,
My intent is to explain the differences as simplistically as possible — something that is not simple at all.
The spinal column is made up of stacked vertebrae: C-1 to C-7 are cervical; T-1 to T-12 are thoracic; L-1 to L-5 are lumbar and S-1 to S- 5 are fused sacral. Pictured from the front or back the column appears straight. Pictured from the side it takes on an S-curve appearance. Pictured from top to bottom it appears as unevenly stacked blocks. Between C-2 and S-1 each vertebral body has a disc — best described as a sponge-like spacer — between it and the next vertebral body. It’s the spinal column body (we call it the anterior element.) that supports 80% of body weight distribution. (The other 20% is handled by the additional posterior facet elements We’ll talk about them later.) In a fully functioning uninjured spinal column each disc is nearly round and the distribution is even.
So what is a disc?
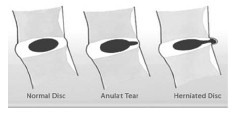
Picture an onion with a jelly bean in the middle. The jelly bean is the nucleus propulsis and it is designed to spread out the force of impact between the two bodies it is cushioning (meaning the vertebral bodies.) All the layers around that jelly bean are the annular rings and they exist to contain the nuclear propulsis.
Adult disc material is avascular meaning that it does not have a blood supply. Cells to remain alive must do two things — eat and flush. Discs are 96% water and function much like a sponge.

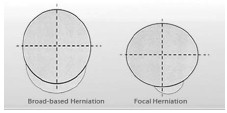
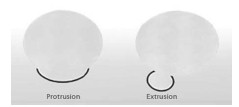
In the case of traumatic injury or of wear and tear the annular rings can weaken or tear. In the case of weakening the jelly bean may bulge. It is possible to have a symetrical bulging disc — in such case the annular walls are symetrically weakened and the material just gets flatter and the disc becomes larger than the two vertebrae it cushions. If the annular rings are weakened mostly in a specific area the bulge is focal in nature (25% or less); a larger area (but less than half; 25- 50%) is called an asymetrical bulging disc. In any of these cases the fluid is still encased between the bodies even if extended. If the annular rings actually tear the jelly bean can leak out and it might then become a disc herniation. Still the fluid that extends outside of the annular rings is contained. A disc is considered ruptured when the leaked mucleus propulsis material — or portion thereof — is no longer a part of what’s left inside.
Again this is highly simplified.
DB
One injured person.
One MRI.
Two radiologists reading the same film and two very different reports. How is this even possible?
Confused in Oregon
Dear Confused, One element that I have long thought the insurance industry is missing within their processing is the understanding that radiologists look at a picture and describe what they see in that picture. Period. While the picture itself is objective, the interpretation of that picture is subjective. The radiologist never sees the patient and has no history. S/he is only looking at a film and commenting upon what s/he sees. The reports generated often contain disclaimers, and given the indisputable fact that the percentage of errors made in finalized/signed radiological reports is disturbingly high (different reports rate this number from a low of 20% — that’s one in five — to a high of 67% — that’s two out of three), both proper patient care and responsible provider judgment demand such clinical verification to assure the best possible chance of correct diagnosis, treatment or compensation.
The injury noted might be more serious than what is reported by the view-only radiologist — or it might be less serious than the buzz words imply. In extreme cases, it could be a genetic malformation, an old football injury, or a normal finding within a particular age group. What one radiologist interprets as a “fracture” might be what another radiologist skips over because he interprets it as a genetic anomaly where there was an incomplete fusing of two bones in an otherwise normal sacrum. There is no right or wrong in matters of interpretation. Finally, be aware that different radiologists may use different words to describe the exact same thing and the only surefire way to determine who got it right is in more extensive diagnostics, an eventual surgeon’s report or … an autopsy report. None of which is ideal, especially the latter! During their extensive training period (generally a four year residency) the basic terminology necessary to translate a visual photo to written language is instilled.
Now pay attention, because this is where it gets tricky.
The radiologist continues to read report after report — for year after year — but his personal interpretation is never altered because he (the radiologist) does not stand next to the surgeon and see the actuality of the real living breathing tissue. Sometimes the surgical report will tell a very different story than that told beforehand by the MRI — but without the input of “here’s what it really was,” the radiologist will continue to see only what he initially saw.
While the American Radiological Association is somewhat clear in acceptable language and terminology usage, the art of photo description can be tricky, errors can occur in the transcription process, and a single world left out (e.g. the word “no”) can have far reaching effects.
The future promises advanced software, programs that are image-linked, that will undoubtedly reduce human error and provide unparalleled language and reporting standardization; but 100% accuracy will not be achievable in the near term. DB
Dear Doctor Bob,
I know that the word “anterior” means front and “posterior” means back. Can you tell me if and when the directional placement of a disc problem and/or the specific size of a bulge needs to be a major consideration in evaluation of an injury?
Mary
Dear Mary,
First, there are no hard fast disc rules that can be applied unilaterally to all patients. Beginning at about age 17 for women and 19- 20 for men, normal growth, fusing, etc., has taken place and the body has completed its initial dervelopment; the individual is as pliable as s/he will ever be. In matters of the spine, the anterior portion of the vertebral bodies is effaced with open space; the posterior portion of the vertebral bodies backs up to the spinal canal, the nerve roots, etc. Thus an individual can have an 8-mm bulge in an anterior position that really doesn’t cause much in the way of symptoms — as opposed to a 2-mm bulge posteriorly that pushes on a nerve and causes intense pain and nonmobility. ‘Tis said that size matters, and of course it does to some degree, but in matters of bulges, herniations, ruptures, etc., placement trumps size in the determination of extent of injury. Simplistically speaking. DB
Dear Dr. Bob,
What is it about the cervical vertebrae and the lower lumbar vertebrae (especially L5-S1) that makes them so susceptible to injury?
Medical Reviewer Reggie
Dear MRR,
Let’s look at this as Anatomy 101 and some basic common sense.
The cervical vertebral bodies are essentially a skinny little stick that must balance and support a 16-pound bowling ball of a head. The human design constantly challenges this area of the body. You hear a sudden noise behind you and you instinctively spin your head to look. The force of a sneeze, all by itself, is equivalent to a low impact collision. Football? Even with a helmet, you’ve got to be kidding. Still, the body and all of the area’s moving/cushioning/protective parts do an amazing collective job in all but extreme situations. Bony structures, muscles, tendons, joints, chemistry, and brain signals all contribute to moment-to-moment protection. Still the stressors are many.
Moving down to all those T’s, you see fewer injuries because the spinal structure in this area provides more protection and flexibility than it does significant movement. The anterior vertebrae are stacked, with posterior elements providing structure, balance, and weight-bearing strength — but T5-T6 (for instance) does not contribute to the body’s ability to bend over and touch the toes.
That’s what L5-S1 does. Primarily, it serves to transfer the weight of the upper body into the pelvis — (sacrum) which is fixed rather than moveable. The place where that transfer is made is pivotal; so stress or injury can come from anywhere. Additionally, it’s where the nerve roots emerge from what is essentially the base of the spinal cord (which ends at L- 2, by the way) — and control the lower extremities. Remember, this one motor unit controls a third of the body, facilitates more fields of movement than any other, and is subject to more traumatic stressors and daily wear and tear than any other portion of the spinal column. Injurious involvement of L4- L-5 is also increased because of the support they provide to the function of L5-S1.
Let’s take a quick detour.
Our bodies, our brains, and our base level circuitry, are built to defend all part of our physical being. Most injuries occur because the response of the body is just not fast enough to cover the unexpected. There’s a lag time, just like a computer has a lag time. Memory chips are instantaneous, however, any time there is a physical entity that has to restrict or extend to protect itself, those micro seconds make a difference. It’s all a part of bio-mechanics, but for now let’s just mention age. In a five-mph car impact (you are stationary, the car hits you) the lag time between being hit and your muscle contraction will open you up to damage. The older you get, the less hydrated you are — and the less elastic as a result. Your reaction time is longer The muscle strength of a 26-year-old is far beyond that of a 62-yearold in almost all cases. Why? Because the activity level of the 62-year-old is not sufficient to keep muscles, tendons, and ligaments as healthy as they might have been 40 years earlier. Older people have a tendency to experience more damage. In fact, the less in shape a person is, the more prone to a higher level of injury in any traumatic incident.
More about this down the line when we talk about the science of bio-mechanics and its relation to injury. I’ve got a word count to adhere to! DB
[color-box color=”gray”]Dr. Bob is an Orthopedic M.D./Surgeon (retired) educated at ASU and USC.[/color-box]Copyright held by The John Cooke Fraud Report. Reprint rights are granted with attribution to The John Cooke Fraud Report with a …
Copyright held by The John Cooke Fraud Report. Reprint rights are granted with attribution to The John Cooke Fraud Report with a …